
Where do we draw our last breath? A comparative analysis of factors associated with places of death in European countries
Article Sidebar
Main Article Content
Abstract
1 INTRODUCTION
One of the greatest human achievements over the past fifty decades has been fighting diseases and improving health care, which has led to increased longevity. However, this increased longevity, combined with decreased fertility rates, has resulted in a larger share of elderly people who need support from an aging and shrinking working-age population (Zweifel, Felder and Meiers 1999;Yang, Norton and Stearns 2003). This demographic shift places a considerable burden on both caregivers and healthcare systems (Hartwig 2008;Howdon and Rice 2018).
Caregivers, predominantly women, often confront significant challenges as they balance personal and professional responsibilities (OECD 2023). This situation frequently necessitates reducing working hours or exiting the workforce altogether, adversely affecting their economic stability and career trajectories (Bauer and Sousa-Poza 2015). This period often aligns with the periods in which their own children require more support, placing these women in what Rosenthal, Martin-Matthews and Matthews (1996) described as the ‘sandwich generation’, trapped between the dual responsibilities of caring for their parents and for their children. This condition is closely associated with heightened poverty rates among informal carers. Furthermore, the physical and emotional demands of caregiving lead to increased healthcare expenditures for caregivers themselves, as they often neglect their own health needs while attending to those of others (Carmichael and Charles 2003;Do et al. 2015).
All of the mentioned factors underscore the necessity for formal long-term care (LTC) services, defined as a range of services required by persons with a reduced degree of functional capacity, physical or cognitive, who are consequently dependent for an extended period of time on help when it comes to basic activities of daily living (ADL) (Ranci and Pavolini 2013). Yet, the diminishing working-age population coupled with a growing demand for LTC is resulting in labour shortages (Costa-Font and Courbage 2012). Therefore, healthcare systems are significantly stressed by these demographic shifts, creating economic challenges that pressure social security and pension systems. Governments and policymakers face the challenge of dedicating more national income to healthcare services, including end-of-life care (EOLC), which refers to the care provided to people who are near the end of life, and long-term care (LTC), while also addressing the uncertainties elderly people face regarding disability and the costs of various care services (OECD 2023).
Understanding the conditions under which people die in different countries can provide policymakers with crucial insights for crafting these policies. This is especially relevant for controlling healthcare costs, given that hospitalisation is generally more expensive than other forms of care (Hoverman et al. 2020). This issue is economically significant and has implications for individual well-being as a 2017 survey by the Organisation for Economic Co-operation and Development (OECD) showed a general aversion to dying in hospital (OECD 2017).
To verify whether a shift to formal LTC, generally accompanied by higher public spending in LTC, is associated with a lower likelihood of dying in hospitals compared to dying at home or in care homes, this study assesses the correspondence between the place of death and a set of demographic, socioeconomic and health variables (Srdelić and Smolić 2022). With the help of multinomial logistic models, we explored the data from the Survey of Health, Ageing and Retirement in Europe (SHARE) database referring to 16,633 individuals aged 50 years and over, who died between 2004 and 2021 in 24 European countries (Börsch-Supan et al. 2013;Börsch-Supan 2022). The countries were divided into two groups to account for variations in healthcare systems across different nations. This categorisation allows for a comparative analysis to shed light on how healthcare financing structures may be associated with the place of death.
The results of this study contribute to the literature on end-of-life care by offering a deeper understanding of the factors associated with the place of death. The research uncovers dynamics in this healthcare decision-making process through a comprehensive analysis of demographic, socioeconomic, health-related, and temporal variables.
The paper begins by providing the research background to outline the motivation for the study. This introduction leads to the methodological section, where data and trends are explored, and the models and methods are detailed. The paper concludes with the presentation of the results, a discussion of the findings, an examination of limitations, and final conclusions.
2 RESEARCH BACKGROUND
Place of death has previously been explored by Orlovic, Marti and Mossialos (2017) in a panel analysis using data from 16 European countries and Israel, utilizing the SHARE database (waves 2 – 5). Our study distinguishes itself in several ways that enhance the analysis and contribute to the existing literature. Firstly, while we draw from the same data source, we focus on a distinct selection of countries. Our primary interest lies in comparing the countries where policymakers support both formal and informal care versus those relying solely on informal care provided by family members, where the only alternative is costly acute care.
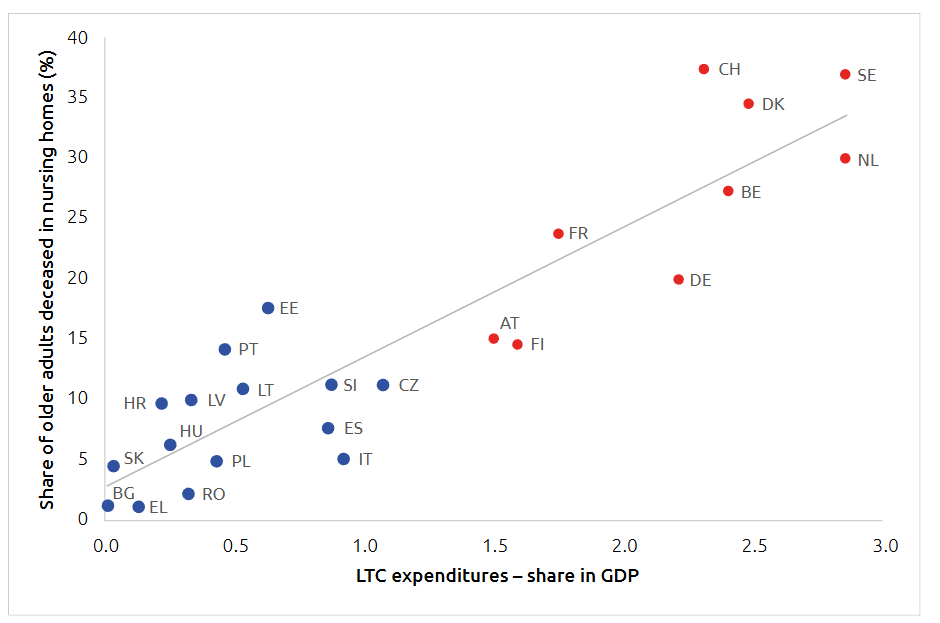
This motivation stems from the data suggesting a strong relationship between the place of death and the level of LTC expenditures in various European countries. According to the Eurostat database on LTC expenditure and SHARE data on place of death, there is a significant positive correlation between LTC spending and the number of individuals aged 50 and over who die in care homes rather than hospitals, as illustrated in Figure 1. The cluster analysis based on these two key variables identified two distinct groups of countries.
Figure 1. Expenditure on LTC (health) in terms of GDP in 2019 and share of deaths in care homes (2004–2021; CG1 in red, CG2 in blue)
Source: Authors calculations based on the Eurostat and SHARE data.
Country Group 1 (CG1) consists of Austria, Belgium, Denmark, Finland, France, Germany, the Netherlands, Sweden, and Switzerland, each allocating over 1.5% of GDP to long-term care (LTC). In these nations, more than 15% of older adult deaths occur in care homes, supported by robust public financing for LTC. Conversely, Country Group 2 (CG2), which includes Bulgaria, Croatia, Czechia, Estonia, Latvia, Lithuania, Greece, Hungary, Italy, Poland, Portugal, Romania, Slovakia, Slovenia, and Spain, lags behind in both LTC funding and the proportion of deaths in care homes, often below the EU-27 average. These 15 countries have less developed LTC systems (Spasova et al. 2018).
Higher LTC expenditures are likely to be associated with the share of elderly who die in nursing homes for several reasons. Firstly, increased expenditures allow for the construction and maintenance of more nursing homes and care facilities, thereby increasing the availability of beds. This ensures that more elderly individuals have access to these facilities, especially in their final years, leading to a higher proportion of deaths occurring in nursing homes.
Secondly, with greater financial resources, nursing homes can invest in better training for staff, advanced medical equipment, and improved living standards for residents. These enhancements in care quality make nursing homes a more attractive option for families and individuals, resulting in higher utilization rates. As incomes rise and societies develop, there is often an increase in expectations regarding the quality and type of care for the elderly. In countries with higher LTC expenditures, elderly may find that professional care in nursing homes can provide better end-of-life care than family-based or informal care. Thirdly, higher public spending on LTC often includes subsidies or financial support for families, making nursing home care more affordable. Increased accessibility ensures that even lower-income families can consider nursing home care as a viable option for their elderly members.
In contrast, countries with lower LTC expenditures may have fewer alternatives for end-of-life care, such as home health care services. This scarcity can force families to rely more on informal caregiving, resulting in a lower share of elderly dying in nursing homes. Countries that invest more in LTC often develop comprehensive policies and infrastructure that support elderly care. This includes integrated healthcare systems that coordinate between hospitals, nursing homes, and home care services to ensure seamless care for the elderly, contributing to higher usage of nursing homes.
3 METHODS
3.1 DATA AND DESCRIPTIVE STATISTICS
The data on 16,633 individuals from 24 European countries is pooled from the End-of-Life questionnaire module of the SHARE project’s waves 2 through 9. SHARE, or the Survey of Health, Ageing and Retirement in Europe, is a cross-national panel database that collects micro data on health, socio-economic status, and social and family networks of individuals aged 50 or older. This comprehensive database covers 28 European countries and Israel, employing face-to-face interviews using a computer-assisted personal interviewing (CAPI) system to gather a wide range of health, economic, and social variables (Börsch-Supan et al. 2013;Börsch-Supan 2022).
This dataset provides detailed information on the last year of the individuals’ lives, including dependency status, time, and cause of death. An ‘End of Life’ interview, which is part of the SHARE project, was conducted solely with family members, or close acquaintances of the deceased respondents to collect comprehensive information on circumstances leading up to the individual’s death. Members of collective households are not included in this sample, focusing exclusively on the individuals who have passed away. These interviews offer valuable insights into the health status changes, care needs, and utilization of health care services in the final years of life, providing a unique perspective on aging and dying in the European context.
The demographic composition of the sample reveals valuable insights (Table 1). For example, a slight majority are male (53.7%) compared to females (46.3%). Age-wise, more than half of the deceased (55.05%) were 80 or older, while the remaining 45.95% were younger than 80. The average age at the time of death was 79.6 years.
| Country | N | Female (%) | Characteristics of deceased persons | Married (%) | |
|---|---|---|---|---|---|
| Mean Age - Female | Mean Age - Male | ||||
| Austria | 762 | 47.4 | 81.2 | 78.1 | 50.8 |
| Belgium | 1060 | 45.0 | 82.6 | 79.4 | 57.4 |
| Bulgaria | 161 | 41.0 | 78.3 | 74.4 | 62.1 |
| Croatia | 432 | 42.8 | 79.6 | 75.7 | 58.6 |
| Czechia | 1193 | 46.9 | 79.3 | 76.4 | 51.1 |
| Denmark | 798 | 49.9 | 81.1 | 79.0 | 46.9 |
| Estonia | 1761 | 46.9 | 81.3 | 76.7 | 54.6 |
| Finland | 55 | 23.6 | 67.1 | 77.7 | 70.9 |
| France | 758 | 46.3 | 83.4 | 79.4 | 55.5 |
| Germany | 586 | 41.1 | 78.1 | 76.5 | 71.8 |
| Greece | 1123 | 53.3 | 84.8 | 81.8 | 44.5 |
| Hungary | 619 | 47.7 | 78.9 | 75.9 | 54.1 |
| Italy | 1113 | 42.9 | 81.0 | 79.2 | 65.9 |
| Latvia | 100 | 47.0 | 80.1 | 71.7 | 49.0 |
| Lithuania | 220 | 53.6 | 79.2 | 72.4 | 47.7 |
| Netherlands | 407 | 43.5 | 77.1 | 77.0 | 76.9 |
| Poland | 959 | 46.3 | 79.1 | 75.7 | 60.5 |
| Portugal | 345 | 48.7 | 80.2 | 75.9 | 57.7 |
| Romania | 270 | 40.0 | 76.1 | 74.4 | 57.4 |
| Slovakia | 89 | 31.5 | 72.4 | 70.9 | 75.3 |
| Slovenia | 848 | 42.3 | 81.5 | 77.5 | 61.8 |
| Spain | 1555 | 48.0 | 84.1 | 80.7 | 54.2 |
| Sweden | 975 | 47.8 | 82.4 | 81.5 | 52.3 |
| Switzerland | 474 | 43.9 | 82.8 | 80.5 | 56.1 |
| Total | 16,663 | 46.3 | 81.3 | 78.1 | 56.1 |
|
Source: authors’ own calculations based on the data from SHARE
Note: C1 in red, C2 in blue. Percentages might not sum to 100 because the categories "other" and "unknown" were omitted. |
|||||
In the research paper, causes of death recorded in the SHARE database have been consolidated into broader categories for more efficient analysis and clearer interpretation, as depicted in Table 2. This categorization aligns closely with the original classifications from the SHARE survey, yet simplifies them into more general groups. The category “Heart attack, stroke or other CVDs” encompasses all cardiovascular-related causes, including heart attacks, strokes, heart failure, and arrhythmia. Cancer directly corresponds to the “Cancer” option in the SHARE questionnaire. The “COVID-19 or other respiratory diseases” category combines deaths due to COVID-19 with other respiratory diseases and severe infectious diseases, such as pneumonia. “Decrepitude, dotage, and senility” were extracted from the broader ‘Other’ category into a standalone group in your analysis due to their high occurrence as causes of death. It encompasses deaths attributed to old age, general decline, or conditions not directly associated with a specific disease pathology. Finally, the “Other” category serves as a catch-all for causes not specified in the primary categories, including accidents and diseases of the digestive system.
| Country (CG1 in red, CG2 in blue) | Hearth attack, stroke or other CVDs | Cancer | Covid-19 or other respiratory diseases | Decrepitude, dosage, senility | Other |
|---|---|---|---|---|---|
| Austria | 37.1 | 21.1 | 4.5 | 7.0 | 30.3 |
| Belgium | 28.8 | 26.5 | 7.2 | 10.2 | 27.4 |
| Bulgaria | 56.5 | 20.5 | 3.7 | 1.9 | 17.4 |
| Croatia | 51.6 | 26.4 | 3.5 | 5.6 | 13.0 |
| Czechia | 42.6 | 24.4 | 4.9 | 9.0 | 19.2 |
| Denmark | 20.9 | 32.8 | 8.5 | 11.9 | 25.8 |
| Estonia | 48.8 | 27.5 | 4.5 | 5.9 | 13.2 |
| Finland | 32.7 | 47.3 | 0.0 | 3.6 | 16.4 |
| France | 29.9 | 32.8 | 7.4 | 8.0 | 21.8 |
| Germany | 31.4 | 32.3 | 4.8 | 4.8 | 26.8 |
| Greece | 59.8 | 17.4 | 9.2 | 2.5 | 11.2 |
| Hungary | 48.9 | 23.1 | 4.2 | 6.9 | 16.8 |
| Italy | 41.2 | 32.6 | 7.5 | 7.5 | 14.6 |
| Latvia | 56.0 | 24.0 | 5.0 | 3.0 | 12.0 |
| Lithuania | 54.1 | 21.8 | 5.5 | 1.4 | 17.3 |
| Netherlands | 23.1 | 38.1 | 4.9 | 4.9 | 29.0 |
| Poland | 48.0 | 27.0 | 7.8 | 5.0 | 12.2 |
| Portugal | 31.6 | 30.4 | 10.4 | 3.5 | 24.1 |
| Romania | 48.5 | 23.7 | 6.3 | 7.0 | 14.4 |
| Slovakia | 46.1 | 37.1 | 14.6 | 0.0 | 2.2 |
| Slovenia | 38.9 | 29.1 | 6.1 | 3.3 | 22.5 |
| Spain | 35.6 | 23.5 | 12.5 | 6.6 | 21.8 |
| Sweden | 31.7 | 31.4 | 5.3 | 12.2 | 19.4 |
| Switzerland | 29.3 | 32.1 | 4.4 | 15.2 | 19.0 |
| Total | 39.8 | 27.3 | 6.8 | 6.8 | 19.3 |
|
Source: authors’ own calculations based on the data from SHARE
Note: Category 'other' includes 'unknown'. |
|||||
The results indicate that cardiovascular diseases (CVDs), such as heart attacks and strokes, were the predominant causes of death, accounting for 39.8% of the sample, as detailed in Table 2. Cancer followed as the second most common cause, affecting 27.3% of the deceased. Interestingly, younger individuals were more prone to dying from cancer, while those 80 and older were more likely to succumb to CVDs. Country-specific data also revealed thought-provoking patterns. For example, Bulgaria had the highest percentage of deaths from heart attacks and strokes (56.5%), whereas Denmark had the lowest (20.9%). On the other hand, Finland had the highest proportion of cancer-related deaths (47.3%), although this should be viewed cautiously due to a small sample size for the country. According to Eurostat data, the principal cause of death across the analysed countries for individuals aged 65 and over is diseases of the circulatory system, or cardiovascular diseases (CVDs) (classified under ICD-10 code “I”), except in Denmark and the Netherlands, where neoplasms, or cancer (classified under ICD-10 codes “C00-D48”), are the predominant causes of death (Eurostat 2023). This aligns with the findings from the SHARE data, thereby reinforcing the reliability of the conclusions drawn from the analysis.
Regarding the location of death, the dataset points to significant differences across countries (Table 3). Hospitals were the most common setting for death in most countries. Still, the percentages ranged widely, from a low of 25% in the Netherlands to as high as 71% in Finland. Care home deaths were most frequent in Switzerland (37.3%), Sweden (36.9%), and Denmark (34.5%). In contrast, home deaths were most common in Bulgaria (78.9%) and Romania (68.9%). These high percentages align with the elevated rates of cardiovascular-related deaths in these countries. However, it is essential to consider other socio-economic factors associated with the place of death in countries like Bulgaria and Romania. The high proportion of home deaths may also be attributed to the inability to cover the costs of care homes, the limited availability of long-term care facilities, and the practice of short hospital stays due to health fund policies, which will be explored further later in the analysis. These factors can be significantly associated with the decision to die at home rather than in institutional settings.
| Country | Hospital | Home | Care Home | |||
|---|---|---|---|---|---|---|
| Total | Female | Total | Female | Total | Female | |
| Austria | 51.8 | 47.1 | 33.1 | 33.0 | 15.1 | 19.9 |
| Belgium | 46.2 | 44.7 | 26.5 | 19.1 | 27.3 | 36.3 |
| Bulgaria | 19.9 | 6.1 | 78.9 | 93.9 | 1.2 | 0.0 |
| Croatia | 48.6 | 47.6 | 41.7 | 41.1 | 9.7 | 11.4 |
| Czechia | 62.2 | 59.1 | 26.6 | 25.4 | 11.2 | 15.5 |
| Denmark | 38.9 | 38.2 | 25.7 | 20.4 | 34.5 | 41.5 |
| Estonia | 45.0 | 41.5 | 37.4 | 34.6 | 17.7 | 23.8 |
| Finland | 70.9 | 84.6 | 14.5 | 15.4 | 14.5 | 0.0 |
| France | 53.6 | 50.7 | 22.7 | 19.7 | 23.7 | 29.6 |
| Germany | 49.0 | 44.4 | 31.1 | 29.0 | 20.0 | 26.6 |
| Greece | 51.6 | 50.7 | 47.2 | 48.2 | 1.2 | 1.2 |
| Hungary | 55.3 | 51.2 | 38.4 | 41.0 | 6.3 | 7.8 |
| Italy | 44.7 | 41.3 | 50.2 | 52.6 | 5.1 | 6.1 |
| Latvia | 35.0 | 44.7 | 55.0 | 38.3 | 10.0 | 17.0 |
| Lithuania | 50.5 | 48.3 | 38.6 | 33.9 | 10.9 | 17.8 |
| Netherlands | 24.6 | 17.5 | 45.5 | 45.2 | 30.0 | 37.3 |
| Poland | 51.1 | 51.1 | 44.0 | 43.2 | 4.9 | 5.6 |
| Portugal | 62.0 | 54.2 | 23.8 | 25.6 | 14.2 | 20.2 |
| Romania | 28.9 | 37.0 | 68.9 | 59.3 | 2.2 | 3.7 |
| Slovakia | 46.1 | 46.4 | 49.4 | 39.3 | 4.5 | 14.3 |
| Slovenia | 57.0 | 53.9 | 31.8 | 28.1 | 11.2 | 18.9 |
| Spain | 56.7 | 54.2 | 35.7 | 36.2 | 7.7 | 9.7 |
| Sweden | 39.5 | 35.2 | 23.6 | 20.4 | 36.9 | 44.4 |
| Switzerland | 39.7 | 40.9 | 23.0 | 15.9 | 37.3 | 43.3 |
| Total | 48.8 | 46.3 | 35.6 | 33.8 | 15.6 | 20.0 |
| CG1 | 44.4 | 41.3 | 27.6 | 23.8 | 28.0 | 35.0 |
| CG2 | 51.2 | 49.0 | 39.9 | 39.1 | 8.8 | 11.9 |
| Source: authors’ own calculations based on the data from SHARE | ||||||
In total, in CG1, 44.4% died in hospitals and 28% in care homes, whereas in CG2, 51.2% died in hospitals and only 8.8% in care homes.
A detailed examination of the place of death for cancer patients reveals significant insights (Table 4). In CG2, the majority of cancer patients (55.8%) died in hospitals, compared to a much lower percentage in CG1, where 47.3% of cancer deaths occurred in hospitals. Interestingly, CG1 had a higher percentage of cancer patients dying in care homes (22%) as compared to CG2 (6.6%).
| Country | Hospital | Home | Care home |
|---|---|---|---|
| Austria | 56.5 | 33.5 | 9.9 |
| Belgium | 56.2 | 27.8 | 16.0 |
| Bulgaria | 15.2 | 84.8 | 0.0 |
| Croatia | 58.8 | 33.3 | 7.9 |
| Czechia | 64.9 | 29.8 | 5.5 |
| Denmark | 41.2 | 32.4 | 26.3 |
| Estonia | 48.2 | 39.4 | 12.4 |
| Finland | 73.1 | 7.7 | 19.2 |
| France | 59.8 | 21.3 | 18.9 |
| Germany | 48.7 | 29.6 | 21.7 |
| Greece | 61.5 | 37.9 | 0.5 |
| Hungary | 67.8 | 26.6 | 5.6 |
| Italy | 46.8 | 49.0 | 4.1 |
| Latvia | 8.3 | 83.3 | 8.3 |
| Lithuania | 60.4 | 25.0 | 14.6 |
| Netherlands | 16.1 | 65.2 | 18.7 |
| Poland | 49.8 | 42.1 | 8.1 |
| Portugal | 80.0 | 11.4 | 8.6 |
| Romania | 20.3 | 76.6 | 3.1 |
| Slovakia | 54.5 | 45.5 | 0.0 |
| Slovenia | 59.9 | 33.2 | 6.9 |
| Spain | 66.0 | 29.9 | 4.1 |
| Sweden | 41.8 | 27.8 | 30.4 |
| Switzerland | 48.0 | 21.7 | 30.3 |
| Total | 52.5 | 34.9 | 12.6 |
| CG1 | 47.3 | 30.7 | 22.0 |
| CG2 | 55.8 | 37.6 | 6.6 |
| Source: authors’ own calculations based on the data from SHARE | |||
3.2 EMPIRICAL STRATEGY AND METHODOLOGY
We adopt multinomial logistic regression models to examine the association between the place of death and other variables. Unlike binary logistic regression, which deals with dependent variables with two categories (like yes or no), multinomial logistic regression handles dependent variables with three or more categories that are not ordered (hospital, home, care home). In the context of this study, the dependent variable is the place of death. We use hospitals as the referent category against which other places of death—homes and care homes—are compared. The outcomes of our multinomial logistic regression models are expressed in terms of Relative Risk Ratios (RRR) in contrast to the previous study’s use of logistic regression and odds ratios (Orlovic, Marti and Mossialos 2017). This shift is crucial because when there is an association between exposure and outcome, OR tends to exaggerate the relationship estimate. Therefore, the interpretation of our results is the following: an RRR greater than 1 suggests that, as a specific variable increases, the outcome is more likely to fall in the comparison group (home, care home), whereas an RRR less than 1 indicates the opposite—higher likelihood of the outcome being in the referent group (hospital).
The independent variables are systematically organized into three categories. Our choice of variables is guided by previous studies that have explored similar questions, reinforcing the robustness of our approach (Cohen et al. 2007;Cohen and Deliens 2012;Pivodic et al. 2015).
First, predisposing factors encompass demographic features such as age and gender and socioeconomic indicators like marital status, number of living children, and home ownership. Second, need-based factors include variables directly related to the individual’s health status, namely the cause of death, duration of illness, and a measure of functional dependency as indicated by the Katz Index. Katz index often referred to as the Katz ADL (Activities of Daily Living) index, is a widely used method in gerontology to assess functional status and the ability of elderly patients to perform basic tasks. Therefore, instead of relying on a single measure of difficulties with ADLs as in Orlovic, Marti and Mossialos (2017), we assess the dependency degree, approximated by the Katz Index (Katz 1983;Costa-Font, Jimenez-Martin and Vilaplana 2018).
Unlike in the research by Orlovic, Marti and Mossialos (2017) who utilised a ‘wave’ as a dummy variable to control for fixed cross-national group differences and secular trends, we employ ‘time’ in this study for the same purposes. ‘Time’ is our temporal variable to capture time trends, divided between 2004–2013 and 2014–2021. The choice to use ‘time’ is motivated by the fact that each wave provides data on patients who passed away in different years (e.g., 2004 and 2014). Therefore, a wave dummy variable cannot adequately capture time-related differences, such as increasing investments in LTC and the rising number of nursing homes over time.
Using these variables, we estimate three models. The first model is a foundational analysis, where we control solely for the country group variable. This is to identify if individuals from specific country groups display a different likelihood of dying at home as opposed to in a hospital or care home. After that we construct two separate models for each country group. These models aim to measure the association of each group’s demographic, socioeconomic, and health-related factors, enabling us to evaluate the divergent relationships of these variables in different national contexts.
For a more mathematical representation, the relative risks associated with different places of death for an individual i are formulated as (Equations 1 and 2):
where the Demo refers to demographic attributes, Soc to socioeconomic traits, Hlth to health-related aspects and the Katz Index, Time stands for the temporal dummy variable, and CG encapsulates the country-specific end-of-life care system characteristics. β coefficients represent the change in the log-odds of the outcome Yi = j relative to the reference category Yi = 0 for a one-unit change in the predictor. The outcome Yi for individual i can take on more than two categories coded as 0, 1, 2 (j = 0, 1, 2). The RRRs tell us by how much the odds of outcome j relative to the reference outcome (0) are multiplied, for each one-unit increase in the predictor variable, while holding other variables constant.
Unlike other regression models, multinomial logistic regression does not require the assumptions of normality, linearity, or homoskedasticity, offering more flexibility (Greene 2018). Nevertheless, it assumes independence among the dependent variable categories. To address this, we utilised the Hausman-McFadden test, a widely accepted method for testing this assumption.
4 RESULTS
Table 5 presents the results of the first model. The intercepts for home and care home indicate the baseline likelihoods when all other factors are at their reference levels. These are substantially less than 1, indicating a lower baseline likelihood of dying in these settings compared to a hospital. Starting with the first block of Demographic characteristics, age does not significantly alter the likelihood of dying at home for those aged 80 and older compared to those aged 50–79, but it substantially increases the likelihood of dying in a care home (RR = 2.244, highly significant). Gender has a small but significantly higher likelihood for females dying in a care home (RR = 1.334, highly significant) compared to males.
| Factor | Home(ref: Hospital) | Care Home(ref: Hospital) |
|---|---|---|
| Intercept | 0.289**** | 0.150**** |
| Demographic characteristics: | ||
| Age 80 and older (ref: 50–79) | 1.045 | 2.244**** |
| Female (ref: Male) | 1.005 | 1.334**** |
| Socioeconomic status and support: | ||
| Married | 1.125*** | 0.622**** |
| Homeownership | 1.025 | 0.748**** |
| N. of children: 0 (ref: 1–2) | 1.147* | 1.149**** |
| N. of children: 3 or more (ref: 1–2) | 1.154**** | 0.851*** |
| Factors related to health: | ||
| Cause of death: Heart attack, stroke or other CVDs(ref: other) | 2.263**** | 1.111 |
| Cause of death: Cancer (ref: other) | 1.546**** | 1.046 |
| Cause of death: COVID-19 or other respiratory disease(ref: other) | 0.847** | 0.689**** |
| Cause of death: Decrepitude, dotage, senility (ref: other) | 4.010**** | 3.103**** |
| Duration of illness: 6m or more (ref: less than 6m) | 1.063 | 1.352**** |
| Katz 1 (ref: Katz 0) | 0.860**** | 1.631**** |
| Katz 2 (ref: Katz 0) | 0.908* | 2.732**** |
| Katz 3 (ref: Katz 0) | 1.257**** | 4.050**** |
| “Year died”: 2014–2021 (ref: 2004–2013) | 1.108*** | 1.288**** |
| CG2 (ref: CG1) | 1.168**** | 0.254**** |
| *p < 0.10 **p < 0.05 ***p < 0.01 ****p < 0.001 | ||
Moving on to the second block, Socioeconomic status and support, being married is associated with a higher likelihood of dying at home (RR = 1.125, highly significant) and a lower likelihood of dying in a care home (RR = 0.622, highly significant). Homeownership is slightly but not statistically significantly associated with dying at home and is associated with a small decrease in the likelihood of dying in a care home (RR = 0.748, highly significant).
Having no children slightly increases the likelihood for both home deaths (RR = 1.147, significant at the 10% level) and care home deaths (RR = 1.149, highly significant). This suggests that individuals without children may lack immediate family caregivers, often relying more on formal care services. Conversely, having three or more children slightly increases the likelihood of dying at home (RR = 1.154, highly significant), but decreases the likelihood of dying in care homes (RR = 0.851, highly significant). This may indicate that larger families provide more potential caregivers, enabling more options for home-based care and reducing reliance on institutional care.
Overall, these findings highlight the complex and context-dependent nature of how socioeconomic status and family structure are associated with the place of death, reflecting varying cultural, social, and economic factors. Regarding our third block of predictor variables – factors related to health, Certain causes of death like heart attacks, strokes, or other cardiovascular diseases significantly increase the likelihood of dying at home (RR = 2.263, highly significant), but not in care homes. Cancer increases the likelihood of dying at home (RR = 1.546, highly significant), but has a negligible effect on care home deaths. Dying from COVID-19 or other respiratory diseases reduces the likelihood in both settings, but more so in care homes (RR = 0.689, highly significant). Conditions associated with frailty, like decrepitude, dotage, or senility, greatly increase the likelihood of dying in care homes (RR = 3.103, highly significant). Duration of illness greater than 6 months is associated with a higher likelihood of dying in a care home (RR = 1.352, highly significant).
Health status, as measured by Activities of Daily Living (ADL) and further detailed by the Katz Index as a scale that measures independence across various daily activities, reveals that the degree of dependency is highly associated with the place of death. Katz 1, indicating mild dependence, reduces the likelihood of dying at home (RR = 0.860, highly significant), but increases it in care homes (RR = 1.631, highly significant). Katz 2, indicating moderate dependence, also reduces the likelihood of ding at home slightly (RR = 0.908, significant at the 10% level), but greatly increases it in care homes (RR = 2.732, highly significant). Katz 3, indicating severe dependence, increases the likelihood of dying at home (RR = 1.257, highly significant), and even more so in care homes (RR = 4.050, highly significant).
Dying in the years 2014–2021, as opposed to 2004–2013, increases the likelihood of dying in both home (RR = 1.108, highly significant) and care home settings (RR = 1.288, highly significant).
Finally, for those in CG 2, there is a significantly increased likelihood of dying at home (RR = 1.168, highly significant), indicating that individuals in this country group are more likely to die at home compared to those in CG1. However, belonging to CG1 is associated with a substantially decreased likelihood of dying in a care home (RR = 0.254, highly significant), suggesting that compared to CG1, individuals in CG2 are less likely to die in care homes.
Table 6 presents a comparative analysis of likelihoods for place of death across two country groups. The baseline likelihoods of dying at home or in a care home are lower than in a hospital for both country groups, with CG2 having the lowest likelihood for care home deaths.
| Factor | Country Group 1 | Country Group 2 | ||
|---|---|---|---|---|
| Home | Care Home | Home | Care Home | |
| Intercept | 0.290**** | 0.136**** | 0.340**** | 0.042**** |
| Demographic characteristics: | ||||
| Age 80 and older (ref: 50–79) | 1.001 | 2.667**** | 1.053**** | 1.727**** |
| Female (ref: Male) | 0.914 | 1.3409**** | 1.032 | 1.343**** |
| Socioeconomic status and support: | ||||
| Married | 1.235*** | 0.658**** | 1.090* | 0.599**** |
| Homeownership | 1.073 | 0.763**** | 0.991 | 0.741**** |
| N. of children: 0 (ref: 1–2) | 1.825 | 1.348*** | 1.142* | 1.703**** |
| N. of children: 3+ (ref: 1–2) | 1.237*** | 0.941 | 1.121** | 0.735**** |
| Factors related to health: | ||||
| Cause of death: Heart attack, stroke or other CVDs(ref: other) | 2.208**** | 1.043 | 2.251**** | 1.121 |
| Cause of death: Cancer (ref: other) | 1.689**** | 1.219** | 1.458**** | 0.840 |
| Cause of death: COVID-19 or other respiratory disease (ref: other) | 1.009 | 0.780* | 0.789** | 0.622*** |
| Cause of death: Decrepitude, dotage, senility (ref: other) | 3.543**** | 3.038**** | 4.315**** | 2.809**** |
| Duration of illness: 6m or more (ref: less than 6m) | 1.053 | 1.197** | 1.064 | 1.597**** |
| Katz 1 (ref: Katz 0) | 0.853* | 1.712**** | 0.871** | 1.546**** |
| Katz 2 (ref: Katz 0) | 0.795** | 3.078**** | 0.963 | 2.226**** |
| Katz 3 (ref: Katz 0) | 1.178* | 4.254**** | 1.299**** | 3.793**** |
| “Year died”: 2014–2021 (ref: 2004–2013) | 1.043 | 1.112 | 1.149** | 1.569**** |
| *p < 0.10 **p < 0.05 ***p < 0.01 ****p < 0.001 | ||||
For demographic characteristics, the age factor shows that in both country groups, individuals aged 80 and older have a significantly higher likelihood of dying in a care home compared to a hospital, with risk ratios of 2.667 and 1.727, respectively. This indicates a pronounced tendency for the very elderly to pass away in care homes rather than hospitals. Gender also appears to play a role, particularly in Country Group 1, where females have 1.3409 times higher likelihood of dying in a care home than males, when compared to the hospital. In Country Group 2, this gender disparity is not significant for deaths at home, but is evident for care home deaths with a risk ratio of 1.343.
Moving on to the second block of predictors – Socioeconomic Status and Support – being married increases the likelihood of dying at home in CG 2 (RR = 1.090) and decreases the likelihood of dying in care homes for both groups. Homeownership is not significantly associated with the likelihood of dying at home, but slightly decreases the likelihood of dying in a care home in both country groups. Having no children increases the likelihood of dying in a care home in both country groups, while having three or more children decreases this likelihood significantly, especially in CG2.
Regarding Factors related to health we observe the following results. Cardiovascular causes of death increase the likelihood of dying at home for both country groups, but have a smaller effect on care home deaths. Cancer increases the likelihood of dying at home significantly in CG1, and to a lesser extent in CG2, with a negligible effect on care home deaths. COVID-19 or other respiratory diseases reduce the likelihood of dying in a care home for both country groups. Decrepitude, dotage, or senility substantially increases the likelihood of dying in a care home for both country groups. A longer duration of illness (6 months or more) increases the likelihood of dying in a care home, particularly in Country Group 2.
As the Katz score increases, indicating higher dependency, there is a decreased likelihood of dying at home but a significantly increased likelihood of dying in a care home for both country groups. The more recent period of 2014–2021 shows an increased likelihood of dying at home for both country groups and in care homes for CG2 compared to the reference period.
5 DISCUSSION
The findings presented in the Results section carry substantial ramifications for healthcare policy, especially for the nations aiming to enhance the quality and environments of end-of-life care. This discussion aims to interpret these findings in the context of existing literature and theoretical frameworks, focusing on implications and potential areas for future research.
The results affirm that age is a significant determinant when it comes to the risk of dying in care homes, particularly for individuals aged 80 and above. This aligns with research suggesting that advanced age is associated with increased care needs, often beyond what can be provided at home (Weaver, Roberto and Brossoie 2020). Gender differences have also been noted, with females experiencing a slightly higher risk of dying in care homes. This may reflect longer life expectancies for women, thus increasing their likelihood of requiring long-term care (Washington et al. 2015;Wong and Phillips 2023).
Socioeconomic factors and support networks are associated in complex ways; the effects differ for each variable and the settings considered (home, hospital, or care home). Overall, being married makes it more likely to die at home and less likely to die in a care home, while owning a home increases the chance of dying at home and decreases the likelihood of dying in a care home. Various models explain this trend, such as altruism and strategic exchange models, suggesting that higher economic status could be associated with the decision-making process for end-of-life care (Courbage and Eeckhoudt 2012;Norton 2000).
Medical conditions and health status are critical determinants of where individuals are likely to die. Patients suffering from cardiovascular diseases (CVDs) and cancer, for instance, are more prone to dying at home, as the predictability and progression of these diseases facilitate better palliative care planning outside of hospitals (Gill, Laporte and Coyte 2018;Ko et al. 2017). A robust primary care system that provides accessible and high-quality services can prevent acute deteriorations in health, thus reducing hospital admissions for these conditions, which are indicators of the quality and accessibility of primary care (OECD 2023). Effective integration between different levels of care for patients with CVDs minimizes unnecessary hospital readmissions and mortality rates, while ensuring proper medication management.
Conversely, conditions that cause high dependency and cognitive decline, such as severe disabilities reflected in higher Katz scores, significantly increase the likelihood of dying in a care home. Previous research supports that severe dependency typically requires professional care that may not be feasible at home (Lysaght and Ersek 2013;Lin et al. 2021).
Hospitals remain the most common setting for death; however, there is a noticeable shift towards more deaths occurring at home or in care homes. This change aligns with findings from a recent OECD (2023), which notes that the share of deaths occurring in hospitals decreased between 2011 and 2021 in many countries, with Denmark and Finland experiencing the largest reductions. Furthermore, during the same period, the proportion of long-term care (LTC) recipients receiving care at home rose significantly, particularly in Switzerland, Finland, and Germany. In Switzerland, the increase in home-based LTC recipients can be attributed to a growth in the availability of home service providers, which has expanded in tandem with the demand for such services. This shift was accelerated during the COVID-19 pandemic, as the crisis led to a temporary reduction in available services, reinforcing a trend that had begun before the pandemic. This information underscores a broader transition in end-of-life care preferences, reflecting a societal move towards more personal and less institutional settings in the final stages of life.
Building on these findings and projections from the OECD (2023), which forecast a doubling in the proportion of the population aged 65 and over, particularly those aged 80 and above, by 2050 in many advanced countries, it is imperative for healthcare systems to adapt to the evolving needs of an aging demographic. This adaptation will likely necessitate an increased demand for labour-intensive long-term care (LTC) and a shift towards integrated, person-centred care models. The COVID-19 crisis highlighted existing workforce shortages in the LTC sector, emphasizing the need for systemic improvements.
Additionally, informal care, primarily provided by women, particularly in South and South-East Europe, is under pressure due to declining family sizes, increased geographic mobility, and rising female labour market participation (OECD 2023). This reduction in available informal caregivers compels countries to expand their formal LTC sectors. While many individuals prefer to remain in their homes, practical limitations such as living alone, or being in remote areas necessitate some transitioning to residential LTC facilities. Therefore, maintaining adequate residential LTC capacity is crucial for effectively addressing the care needs of the aging population.
6 CONCLUSION
This article advances the international literature on end-of-life care. By exploring the dynamics of formal long-term care (LTC) expenditure and its relationship to places of death across different European settings, this study integrates a comprehensive dataset from the Survey of Health, Ageing, and Retirement in Europe (SHARE), covering 16,633 individuals from 24 European countries over the period from 2004 to 2021.
Key advancements of this research include a comparative analysis across country groups, based on their LTC funding levels. This analysis provides insights into how different healthcare financing structures are associated with the location of death, thereby offering valuable information that can inform policy formulations in aging European societies. By employing multinomial logistic regression models, the study not only assesses demographic and socio-economic factors, but it also incorporates health-related variables, thus offering a more detailed picture of the factors influencing end-of-life care locations than previous studies.
The study further integrates health status and LTC context by including health-related characteristics such as the cause of death and the Katz Index of independence. Additionally, the research updates and expands previous analyses by considering a broader timeframe and including a wider array of European countries. This analytical framework allows for the examination of potential shifts towards dying at home or in care homes instead in hospitals, reflecting broader trends in healthcare preferences and LTC availability.
By addressing these dimensions, the paper not only contributes to the academic discourse on aging and healthcare, but also provides practical, data-driven insights that can inform future healthcare policies and LTC planning in Europe. These contributions are vital for enhancing the understanding of end-of-life care dynamics and are crucial for shaping effective and compassionate healthcare policies. Moving forward, future research is recommended to ensure a more equitable distribution of sample sizes across different nations. Specifically, while the current dataset included a substantial number of individuals in total, the variance in sample sizes—ranging from as few as 55 in Finland to over 1,700 in Estonia—could potentially skew the comparative analysis across the 24 countries involved. Balancing the datasets would likely provide a more robust framework for understanding the complex factors associated with end-of-life care decisions. Future studies could also further delineate the causal relationships between these factors and end-of-life care options, while also assessing the role of new healthcare models and evolving policies.
This work was previously published as a working paper in the SHARE Working Paper Series 83-2022 (DOI:
Data availability statement
Data are available from the author upon request.
References
- Bauer, J. M., & Sousa-Poza, A. (2015). Impacts of Informal Caregiving on Caregiver Employment, Health, and Family. Population Ageing, 8, 113–145. https://doi.org/10.1007/s12062-015-9116-0
- Börsch-Supan, A., Brandt, M., Hunkler, C., Kneip, T., Korbmacher, J., Malter, F., … Zuber, S. (2013). Data resource profile: The survey of health, ageing and retirement in Europe (SHARE). International Journal of Epidemiology, 42(4), 992–1001. https://doi.org/10.1093/ije/dyt088
- Börsch-Supan, A. (2022). Survey of Health, Ageing and Retirement in Europe (SHARE) Waves 1–8 and COVID-19 Survey 2 (Wave 9). Release version: 8.0.0. SHARE-ERIC. Data set. https://doi.org/10.6103/SHARE.w1.800 ; https://doi.org/10.6103/SHARE.w2.800 ; https://doi.org/10.6103/SHARE.w3.800 ; https://doi.org/10.6103/SHARE.w4.800 ; https://doi.org/10.6103/SHARE.w5.800 ; https://doi.org/10.6103/SHARE.w6.800 ; https://doi.org/10.6103/SHARE.w7.800 ; https://doi.org/10.6103/SHARE.w8.800 ; https://doi.org/10.6103/SHARE.w9ca.800
- Carmichael, F., & Charles, S. (2003). The opportunity costs of informal care: does gender matter? Journal of Health Economics, 22 (5), 781–803. https://doi.org/10.1016/S0167-6296(03)00044-4
- Cohen, J., Bilsen, J., Fischer, S., Löfmark, R., Norup, M., van der Heide, A., … Deliens, L. (2007). End-of-life decision-making in Belgium, Denmark, Sweden and Switzerland: Does place of death make a difference? Journal of Epidemiology and Community Health, 61(12), 1062–1068. https://doi.org/10.1136/jech.2006.056341
- Cohen, J., & Deliens, L. (Ed.). (2012). A public health perspective on end-of-life care. Oxford: Oxford University Press. https://doi.org/10.1093/acprof:oso/9780199599400.001.0001
- Costa-Font, J., & Courbage, C. (Ed.). (2012). Financing Long-Term Care in Europe: Institutions, Markets and Models. New York: Palgrave Macmillan.
- Costa-Font, J., Jimenez-Martin, S., & Vilaplana, C. (2018). Does long-term care subsidisation reduce hospital admissions and utilisation? Journal of Health Economics, 58, 43–66. https://doi.org/10.1016/j.jhealeco.2018.01.002
- Courbage, C., & Eeckhoudt, L. (2012). On insuring and caring for parents’ long-term care needs. Journal of Health Economics, 31(6), 842–850. https://doi.org/10.1016/j.jhealeco.2012.08.001
- Do, Y. K., Norton, E. C., Stearns, S. C., & Van Houtven, C. H. (2015). Informal care and caregiver’s health. Health Economics, 24(2), 224–237. https://doi.org/10.1002/hec.3012
- Eurostat (2023). Causes of death statistics. https://doi.org/10.2908/HLTH_CD_ARO
- Gill, A., Laporte, A., & Coyte, P. C. (2018). Predictors of home death in palliative care patients: A critical literature review. Journal of Palliative Care, 29(2), 113–118. https://doi.org/10.1177/082585971302900208
- Greene, W. H. (2018). Econometric Analysis (8th ed.) London: Pearson.
- Hartwig, J. (2008). What drives health care expenditure? Baumol’s model of’ unbalanced growth’ revisited. Journal of Health Economics, 27(3), 603–23. https://doi.org/10.1016/j.jhealeco.2007.05.006
- Hoverman, J. R., Mann, B. B., Phu, S., Nelson, P., Hayes, J. E., Taniguchi, C. B., & Neubauer, M. A. (2020). Hospice or hospital: The costs of dying of cancer in the oncology care model. Palliative Medicine Reports, 1(1), 92–96. https://doi.org/10.1089/pmr.2020.0023
- Howdon, D., & Rice, N. (2018). Health care expenditures, age, proximity to death and morbidity: Implications for an ageing population. Journal of Health Economics, 57, 60–74. https://doi.org/10.1016/j.jhealeco.2017.11.001
- Katz, S. (1983). Assessing self-maintenance: Activities of daily living, mobility, and instrumental activities of daily living. Journal of the American Geriatrics Society, 31(12), 721–727. https://doi.org/10.1111/j.1532-5415.1983.tb03391.x
- Ko, M.-C., Huang, S.-J., Chen, C.-C., Chang, Y.-P., Lien, H.-Y., Lin, J.-Y., … Chan, S.-Y. (2017). Factors predicting a home death among home palliative care recipients. Medicine (Baltimore), 96(41), e8210. https://doi.org/10.1097/MD.0000000000008210
- Lin, C.-P., Tsay, M.-S., Chang, Y.-H., Chen, H.-C., Wang, C.-Y., Chuang, Y.-S., & Wu, C.-Y. (2021). A comparison of the survival, place of death, and medical utilization of terminal patients receiving hospital-based and community-based palliative home care: A retrospective and propensity score matching cohort study. International Journal of Environmental Research and Public Health, 18(14), 7272. https://doi.org/10.3390/ijerph18147272
- Lysaght, S., & Ersek, M. (2013). Settings of care within hospice: New options and questions about dying “at home.” Journal of Hospice & Palliative Nursing, 15(3), 171–176. https://doi.org/10.1097/NJH.0b013e3182765a17
- Norton, E. (2000). Long-term care. In A. J. Culyer, & J. P. Newhouse (Eds.), Handbooks of Health Economics (pp. 955–994). Amsterdam: North Holland. http://dx.doi.org/10.1016/S1574-0064(00)80030-X
- OECD (2017). Health at a Glance 2017: OECD Indicators. Paris: OECD Publishing https://doi.org/10.1787/health_glance-2017-en
- OECD (2023). Health at a Glance 2023: OECD Indicators. Paris: OECD Publishing https://doi.org/10.1787/7a7afb35-en
- Orlovic, M., Marti, J., & Mossialos, E. (2017). Analysis Of End-Of-Life Care, Out-Of-Pocket Spending, And Place Of Death In 16 European Countries And Israel. Health Affairs, 36(7), 1201–1210. https://doi.org/10.1377/hlthaff.2017.0166
- Pivodic, L., Pardon, K., Morin, L., Addington-Hall, J., Miccinesi, G., Cardenas-Turanzas, M., … Cohen, J. (2015). Place of death in the population dying from diseases indicative of palliative care need: A cross-national population-level study in 14 countries. Journal of Epidemiology and Community Health, 70(1), 17–24. https://doi.org/10.1136/jech-2014-205365
- Ranci, C., & Pavolini, E. (Eds.). (2013). Reforms in Long-Term Care Policies in Europe: Investigating Institutional Change and Social Impacts. New York: Springer. https://link.springer.com/book/10.1007/978-1-4614-4502-9
- Rosenthal, C. J., Martin-Matthews, A., & Matthews, S. H. (1996). Caught in the Middle? Occupancy in Multiple Roles and Help to Parents in a National Probability Sample of Canadian Adults. Journals of Gerontology: Series B, Psychological Sciences and Social Sciences, 51(6), S274-S283. https://doi.org/10.1093/geronb/51b.6.s274
- Spasova, S., Baeten, R., Coster, S., Ghailani, D., Peña-Casas, R., & Vanhercke, B. (2018). Challenges in long-term care in Europe: A study of national policies. European Social Policy Network (ESPN), Brussels: European Commission.
- Srdelić, L., & Smolić, S. (2022). Factors associated with place of death: evidence from older adults in 24 European countries. SHARE Working Paper Series 83–2022, preprint. https://doi.org/10.17617/2.3477442
- Washington, K. T., Pike, K. C., Demiris, G., Parker Oliver, D., Albright, D. L., & Lewis, A. M. (2015). Gender differences in caregiving at end of life: Implications for hospice teams. Journal of Palliative Medicine, 18(12), 1048–1053. https://doi.org/10.1089/jpm.2015.0214
- Weaver, R. H., Roberto, K. A., & Brossoie, N. (2020). A scoping review: Characteristics and outcomes of residents who experience involuntary relocation. The Gerontologist, 60(1), e20–e37. https://doi.org/10.1093/geront/gnz035
- Wong, A. D., & Phillips, S. P. (2023). Gender disparities in end of life care: A scoping review. Journal of Palliative Care, 38(1), 78–96. https://doi.org/10.1177/08258597221120707
- Yang, Z., Norton, E. C., & Stearns, S. C. (2003). Longevity and Health Care Expenditures: The Real Reasons Older People Spend More. The Journals of Gerontology Series B, 58(1), S2–S10. https://doi.org/10.1093/geronb/58.1.s2
- Zweifel, P., Felder, S., & Meiers, M. (1999). Ageing of population and health care expenditure: a red herring? Health Economics, 8(6), 485–496. https://doi.org/10.1002/(sici)1099-1050(199909)8:6<485::aid-hec461>3.0.co;2-4
Article Details
Published by the Institute of Social Sciences - Center for Demographic Research




References
Bauer, J. M., & Sousa-Poza, A. (2015). Impacts of Informal Caregiving on Caregiver Employment, Health, and Family. Population Ageing, 8, 113–145. https://doi.org/10.1007/s12062-015-9116-0 DOI: https://doi.org/10.1007/s12062-015-9116-0
Börsch-Supan, A., Brandt, M., Hunkler, C., Kneip, T., Korbmacher, J., Malter, F., … Zuber, S. (2013). Data resource profile: The survey of health, ageing and retirement in Europe (SHARE). International Journal of Epidemiology, 42(4), 992–1001. https://doi.org/10.1093/ije/dyt088 DOI: https://doi.org/10.1093/ije/dyt088
Börsch-Supan, A. (2022). Survey of Health, Ageing and Retirement in Europe (SHARE) Waves 1-8 and COVID-19 Survey 2 (Wave 9). Release version: 8.0.0. SHARE-ERIC. Data set. https://doi.org/10.6103/SHARE.w1.800; https://doi.org/10.6103/SHARE.w2.800; https://doi.org/10.6103/SHARE.w3.800; https://doi.org/10.6103/SHARE.w4.800; https://doi.org/10.6103/SHARE.w5.800; https://doi.org/10.6103/SHARE.w6.800; https://doi.org/10.6103/SHARE.w7.800; https://doi.org/10.6103/SHARE.w8.800; https://doi.org/10.6103/SHARE.w9ca.800
Carmichael, F., & Charles, S. (2003). The opportunity costs of informal care: does gender matter? Journal of Health Economics, 22 (5), 781-803. https://doi.org/10.1016/S0167-6296(03)00044-4 DOI: https://doi.org/10.1016/S0167-6296(03)00044-4
Cohen, J., Bilsen, J., Fischer, S., Löfmark, R., Norup, M., van der Heide, A., … Deliens, L. (2007). End-of-life decision-making in Belgium, Denmark, Sweden and Switzerland: Does place of death make a difference? Journal of Epidemiology and Community Health, 61(12), 1062-1068. https://doi.org/10.1136/jech.2006.056341 DOI: https://doi.org/10.1136/jech.2006.056341
Cohen, J., & Deliens, L. (Ed.). (2012). A public health perspective on end-of-life care. Oxford: Oxford University Press. https://doi.org/10.1093/acprof:oso/9780199599400.001.0001 DOI: https://doi.org/10.1093/acprof:oso/9780199599400.001.0001
Costa-Font, J., & Courbage, C. (Ed.). (2012). Financing Long-Term Care in Europe: Institutions, Markets and Models. New York: Palgrave Macmillan. DOI: https://doi.org/10.1057/9780230349193
Costa-Font, J., Jimenez-Martin, S., & Vilaplana, C. (2018). Does long-term care subsidisation reduce hospital admissions and utilisation? Journal of Health Economics, 58, 43-66. https://doi.org/10.1016/j.jhealeco.2018.01.002 DOI: https://doi.org/10.1016/j.jhealeco.2018.01.002
Courbage, C., & Eeckhoudt, L. (2012). On insuring and caring for parents’ long-term care needs. Journal of Health Economics, 31(6), 842-850. https://doi.org/10.1016/j.jhealeco.2012.08.001 DOI: https://doi.org/10.1016/j.jhealeco.2012.08.001
Do, Y. K., Norton, E. C., Stearns, S. C., & Van Houtven, C. H. (2015). Informal care and caregiver’s health. Health Economics, 24(2), 224-237. https://doi.org/10.1002/hec.3012 DOI: https://doi.org/10.1002/hec.3012
Eurostat (2023). Causes of death statistics. https://doi.org/10.2908/HLTH_CD_ARO
Gill, A., Laporte, A., & Coyte, P. C. (2018). Predictors of home death in palliative care patients: A critical literature review. Journal of Palliative Care, 29(2), 113–118. https://doi.org/10.1177/082585971302900208 DOI: https://doi.org/10.1177/082585971302900208
Greene, W. H. (2018). Econometric Analysis (8th ed.) London: Pearson.
Hartwig, J. (2008). What drives health care expenditure? Baumol’s model of’ unbalanced growth’ revisited. Journal of Health Economics, 27(3), 603–23. https://doi.org/10.1016/j.jhealeco.2007.05.006 DOI: https://doi.org/10.1016/j.jhealeco.2007.05.006
Hoverman, J. R., Mann, B. B., Phu, S., Nelson, P., Hayes, J. E., Taniguchi, C. B., & Neubauer, M. A. (2020). Hospice or hospital: The costs of dying of cancer in the oncology care model. Palliative Medicine Reports, 1(1), 92–96. https://doi.org/10.1089/pmr.2020.0023 DOI: https://doi.org/10.1089/pmr.2020.0023
Howdon, D., & Rice, N. (2018). Health care expenditures, age, proximity to death and morbidity: Implications for an ageing population. Journal of Health Economics, 57, 60–74. https://doi.org/10.1016/j.jhealeco.2017.11.001 DOI: https://doi.org/10.1016/j.jhealeco.2017.11.001
Katz, S. (1983). Assessing self-maintenance: Activities of daily living, mobility, and instrumental activities of daily living. Journal of the American Geriatrics Society, 31(12), 721–727. https://doi.org/10.1111/j.1532-5415.1983.tb03391.x DOI: https://doi.org/10.1111/j.1532-5415.1983.tb03391.x
Ko, M.-C., Huang, S.-J., Chen, C.-C., Chang, Y.-P., Lien, H.-Y., Lin, J.-Y., … Chan, S.-Y. (2017). Factors predicting a home death among home palliative care recipients. Medicine (Baltimore), 96(41), e8210. https://doi.org/10.1097/MD.0000000000008210 DOI: https://doi.org/10.1097/MD.0000000000008210
Lin, C.-P., Tsay, M.-S., Chang, Y.-H., Chen, H.-C., Wang, C.-Y., Chuang, Y.-S., & Wu, C.-Y. (2021). A comparison of the survival, place of death, and medical utilization of terminal patients receiving hospital-based and community-based palliative home care: A retrospective and propensity score matching cohort study. International Journal of Environmental Research and Public Health, 18(14), 7272. https://doi.org/10.3390/ijerph18147272 DOI: https://doi.org/10.3390/ijerph18147272
Lysaght, S., & Ersek, M. (2013). Settings of care within hospice: New options and questions about dying "at home." Journal of Hospice & Palliative Nursing, 15(3), 171–176. https://doi.org/10.1097/NJH.0b013e3182765a17 DOI: https://doi.org/10.1097/NJH.0b013e3182765a17
Norton, E. (2000). Long-term care. In A. J. Culyer, & J. P. Newhouse (Eds.), Handbooks of Health Economics (pp. 955-994). Amsterdam: North Holland. http://dx.doi.org/10.1016/S1574-0064(00)80030-X DOI: https://doi.org/10.1016/S1574-0064(00)80030-X
OECD (2017). Health at a Glance 2017: OECD Indicators. Paris: OECD Publishing
https://doi.org/10.1787/health_glance-2017-en DOI: https://doi.org/10.1787/health_glance-2017-en
OECD (2023). Health at a Glance 2023: OECD Indicators. Paris: OECD Publishing https://doi.org/10.1787/7a7afb35-en DOI: https://doi.org/10.1787/7a7afb35-en
Orlovic, M., Marti, J., & Mossialos, E. (2017). Analysis Of End-Of-Life Care, Out-Of-Pocket Spending, And Place Of Death In 16 European Countries And Israel. Health Affairs, 36(7), 1201-1210. https://doi.org/10.1377/hlthaff.2017.0166 DOI: https://doi.org/10.1377/hlthaff.2017.0166
Pivodic, L., Pardon, K., Morin, L., Addington-Hall, J., Miccinesi, G., Cardenas-Turanzas, M., … Cohen, J. (2015). Place of death in the population dying from diseases indicative of palliative care need: A cross-national population-level study in 14 countries. Journal of Epidemiology and Community Health, 70(1), 17-24. https://doi.org/10.1136/jech-2014-205365 DOI: https://doi.org/10.1136/jech-2014-205365
Ranci, C., & Pavolini, E. (Eds.). (2013). Reforms in Long-Term Care Policies in Europe: Investigating Institutional Change and Social Impacts. New York: Springer. https://link.springer.com/book/10.1007/978-1-4614-4502-9 DOI: https://doi.org/10.1007/978-1-4614-4502-9
Rosenthal, C. J., Martin-Matthews, A., & Matthews, S. H. (1996). Caught in the Middle? Occupancy in Multiple Roles and Help to Parents in a National Probability Sample of Canadian Adults. Journals of Gerontology: Series B, Psychological Sciences and Social Sciences, 51(6), S274-S283. https://doi.org/10.1093/geronb/51b.6.s274 DOI: https://doi.org/10.1093/geronb/51B.6.S274
Spasova, S., Baeten, R., Coster, S., Ghailani, D., Peña-Casas, R., & Vanhercke, B. (2018). Challenges in long-term care in Europe: A study of national policies. European Social Policy Network (ESPN), Brussels: European Commission.
Srdelić, L., & Smolić, S. (2022). Factors associated with place of death: evidence from older adults in 24 European countries. SHARE Working Paper Series 83-2022, preprint. https://doi.org/10.17617/2.3477442
Washington, K. T., Pike, K. C., Demiris, G., Parker Oliver, D., Albright, D. L., & Lewis, A. M. (2015). Gender differences in caregiving at end of life: Implications for hospice teams. Journal of Palliative Medicine, 18(12), 1048–1053. https://doi.org/10.1089/jpm.2015.0214 DOI: https://doi.org/10.1089/jpm.2015.0214
Weaver, R. H., Roberto, K. A., & Brossoie, N. (2020). A scoping review: Characteristics and outcomes of residents who experience involuntary relocation. The Gerontologist, 60(1), e20–e37. https://doi.org/10.1093/geront/gnz035 DOI: https://doi.org/10.1093/geront/gnz035
Wong, A. D., & Phillips, S. P. (2023). Gender disparities in end of life care: A scoping review. Journal of Palliative Care, 38(1), 78–96. https://doi.org/10.1177/08258597221120707 DOI: https://doi.org/10.1177/08258597221120707
Yang, Z., Norton, E. C., & Stearns, S. C. (2003). Longevity and Health Care Expenditures: The Real Reasons Older People Spend More. The Journals of Gerontology Series B, 58(1), S2–S10. https://doi.org/10.1093/geronb/58.1.s2 DOI: https://doi.org/10.1093/geronb/58.1.S2
Zweifel, P., Felder, S., & Meiers, M. (1999). Ageing of population and health care expenditure: a red herring? Health Economics, 8(6), 485–496. https://doi.org/10.1002/(sici)1099-1050(199909)8:6<485::aid-hec461>3.0.co;2-4 DOI: https://doi.org/10.1002/(SICI)1099-1050(199909)8:6<485::AID-HEC461>3.0.CO;2-4